Ancient Plague, Antioxidant Genetics, and the ReBalU Test→Treat→Test Platform


A Precision-Medicine Framework for Redox-Fragile Populations
Core thesis: Historic pathogen pressure, including plague, may have shaped population-level immune and redox differences, while modern clinical development remains overly dependent on European-ancestry biology. ReBalU proposes a genotype- and biomarker-guided way to identify redox-fragile individuals and restore endogenous butyrate/DHA signaling to improve cellular resilience and therapeutic responsiveness.
The Plague That Rewired Human Immunity
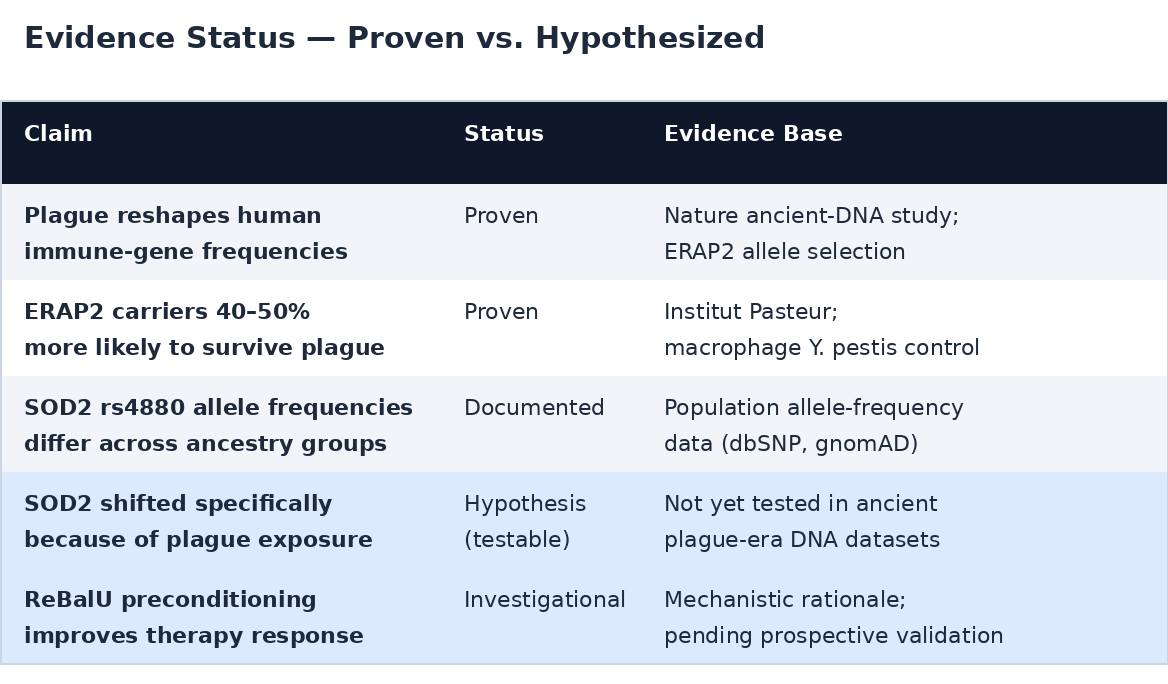
The Black Death provides proof that infectious pressure can rapidly alter human immune-genetic architecture. A Nature ancient-DNA study examined 206 ancient DNA extracts from London and Denmark — before, during, and after the Black Death — and identified immune loci with strong differentiation, including ERAP2, NFATC1, CTLA4, and TICAM2/TMED7.
The ERAP2 result is the strongest model for this paper: the selected allele was associated with full-length ERAP2 transcript production, altered cytokine response to Y. pestis, and improved control of intracellular Y. pestis in macrophages. Institut Pasteur summarized the same work by noting that protective ERAP2 alleles allowed more efficient neutralization of Y. pestis and that carriers were estimated to be 40% to 50% more likely to survive.
But plague didn’t just reshape antigen presentation. Y. pestis forces a macrophage and neutrophil redox battle: host cells use ROS/RNS for antimicrobial killing, while Y. pestis expresses its own stress-response systems to survive inside host compartments. That battle puts a premium on the host’s antioxidant machinery — and specifically on SOD2.
The Redox-Resilience Hypothesis
SOD2 rs4880 is a logical candidate for evolutionary study because its T allele encodes valine at codon 16, and the Val/Val (TT) genotype reduces mitochondrial superoxide-handling efficiency by 30–40%. Population allele-frequency data show that rs4880 differs across ancestry groups — near 0.50 in Europeans, ~0.58 in African ancestry, and near-fixed (TT) in East Asians.
The extension from proven immune selection to redox-resilience selection is plausible: populations repeatedly exposed to plague, parasites, bacteria, viruses, and famine-like stress may have undergone selection not only in antigen-presentation genes, but also in antioxidant-response systems — SOD2, GPX1, GPX4, glutathione metabolism, APOE biology, ferroptosis control, and butyrate/DHA-dependent immune regulation.
The critical scientific distinction: ERAP2 has direct plague ancient-DNA evidence. SOD2 rs4880 does not — yet. The plague-specific claim remains a testable hypothesis, not a proven finding. A scientifically defensible paper must separate the two.
How Pathogens and Cancer Hijack the Same Systems
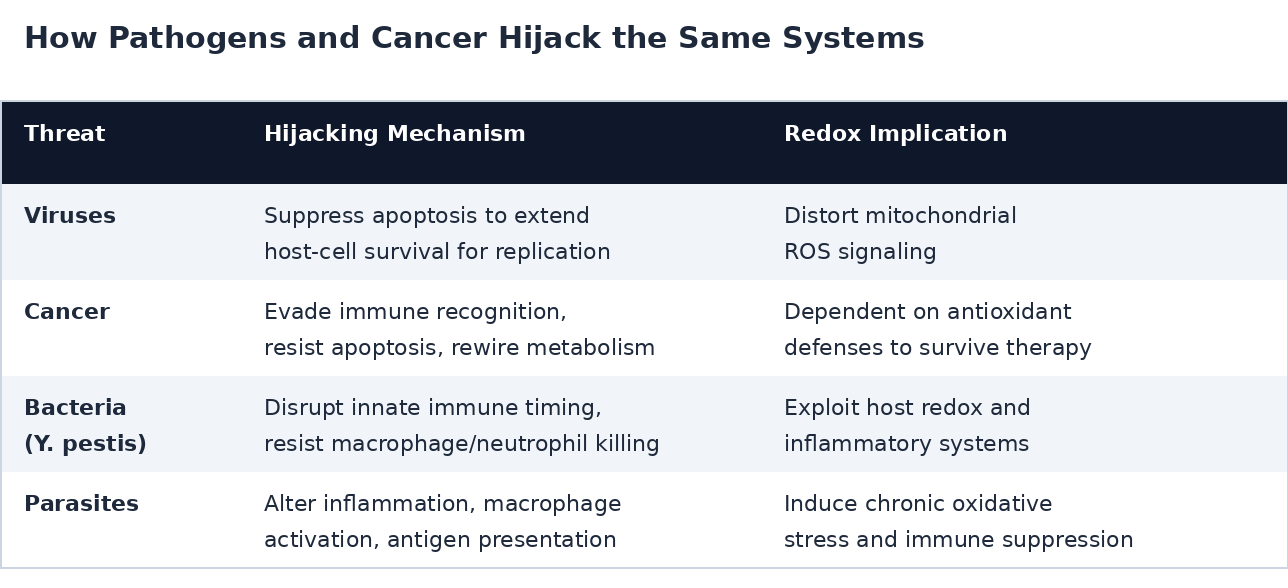
Cancer, viruses, bacteria, and parasites survive by manipulating host-cell survival systems rather than simply attacking from outside. The common biological pattern is hijacking of apoptosis, antigen presentation, mitochondrial metabolism, ferroptosis control, immune checkpoints, cytokine signaling, oxidative stress, and macrophage/T-cell communication.
Viruses must manipulate apoptotic pathways to extend host-cell survival long enough to replicate. Cancer cells evade immune recognition, resist apoptosis, and often become dependent on antioxidant-defense systems to survive therapy. Ferroptosis is now seen as a way to bypass traditional apoptosis resistance — killing cells through iron-dependent lipid-peroxide accumulation and exposing metabolic vulnerabilities in drug-resistant cancers.
Y. pestis fits this model because it survives by disrupting innate immune timing, resisting macrophage/neutrophil killing, and exploiting host redox and inflammatory systems. The plague story becomes a model for a broader principle: redox-fragile hosts may be harmed not only by the pathogen, but also by the host’s own emergency ROS/RNS response — and by oxidative stress added by some bactericidal therapies.
The Precision-Medicine Blind Spot
Modern drug development creates a structural blind spot because clinical and genomic evidence bases remain heavily European-biased. GWAS participants were 86.3% European ancestry as of June 2021, and more than 94% of genomic material available to scientists is European ancestry. FDA 2020 drug-approval trial data were 75% White, and drugs historically were tested primarily on White men — creating uncertainty in safety and efficacy for underrepresented populations.
This matters for redox genetics because the protective C(Ala) allele is most common in European populations (~25% CC, ~50% TC). Anchoring “normal” antioxidant reference ranges to the one group with the highest rate of the protective allele dilutes true TT-driven effects toward null — and likely underestimates the real magnitude of redox fragility in the global majority.
The ReBalU Protocol
Identify: The Genetic and Biomarker Panel
The ReBalU Test→Treat→Test protocol identifies individuals whose antioxidant systems are genetically or biochemically fragile before they encounter severe infection, cancer therapy, chronic inflammatory disease, or drug-induced oxidative stress.
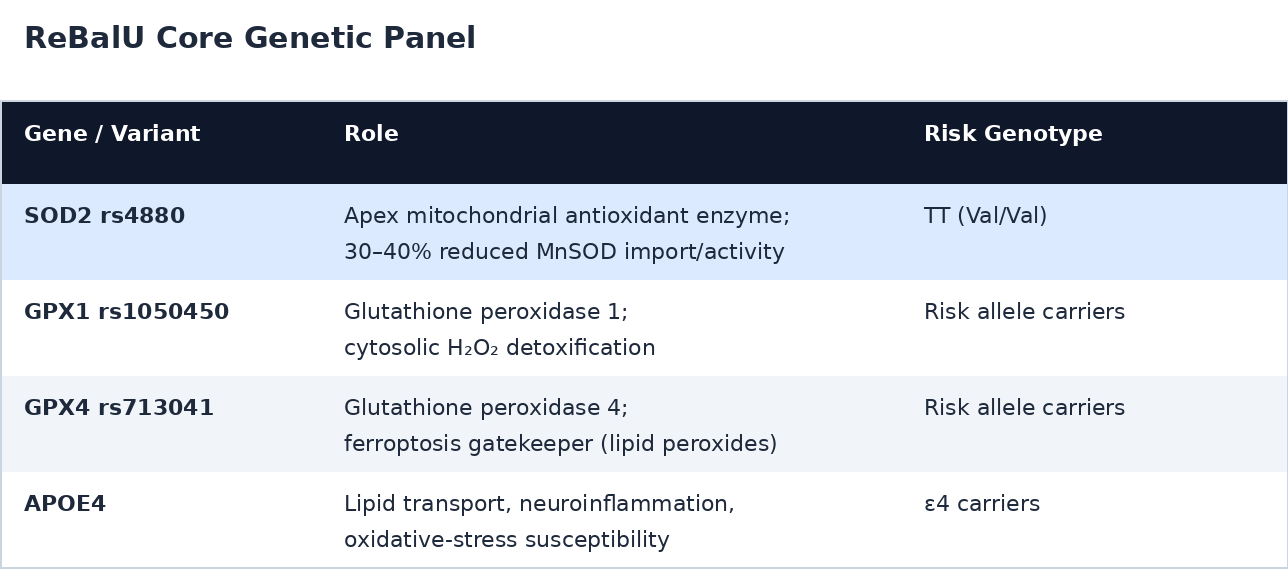
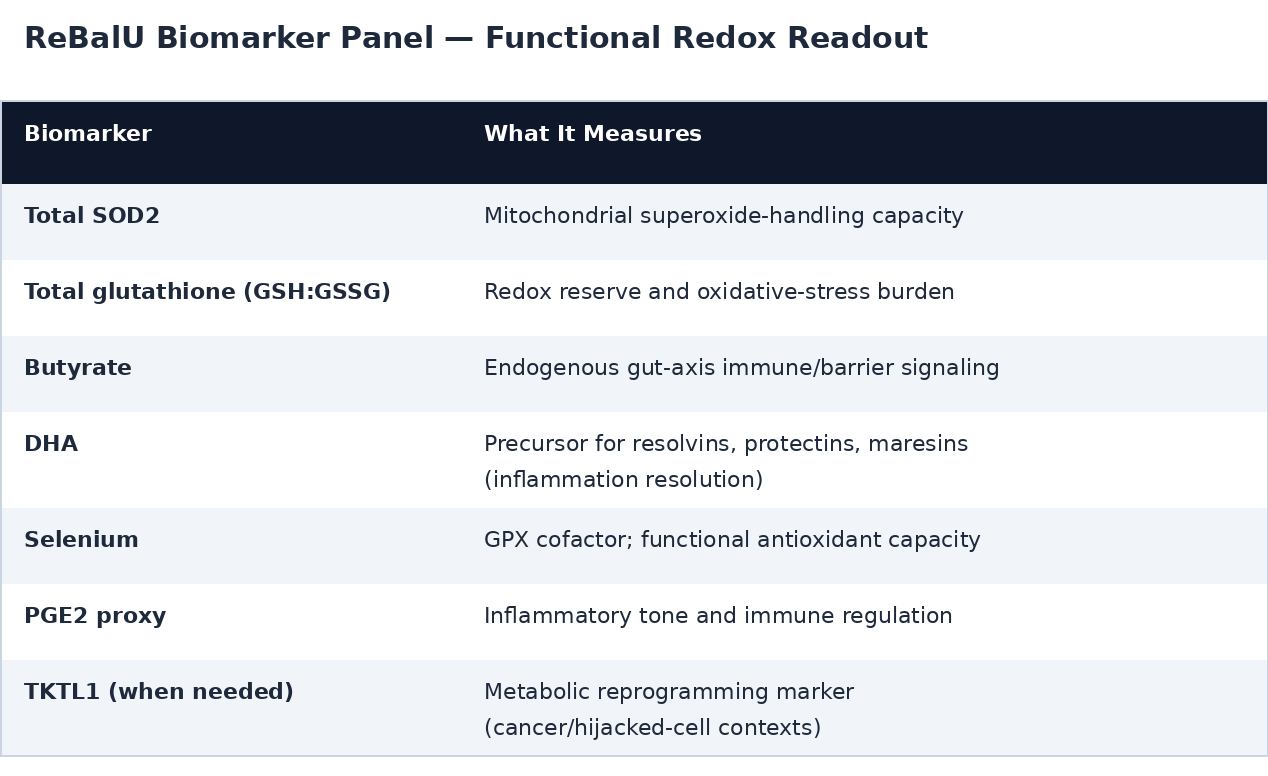
Genotype creates predisposition, but phenotype determines whether the person is currently resilient, compensated, or depleted. The biomarker panel measures redox reserve and pathway function rather than genotype alone:
Treat: Endogenous Butyrate/DHA Restoration
The ReBalU gummy and mouthwash protocol is not a sodium-butyrate bolus strategy. It is a repeated endogenous butyrate-generation and DHA co-delivery platform — 2 gummies three times daily plus morning/evening mouthwash exposure to support continuous mouth-gut-axis conditioning.
The distinction from direct sodium-butyrate supplementation is critical. Microbiota-generated butyrate is produced at the colonic epithelial and mucosal immune interface, where it fuels colonocytes, supports gut-barrier integrity, and modulates immune-cell programming before only lower amounts reach portal or systemic circulation. ReBalU generates butyrate in situ through fermentation — continuous local physiologic signaling, not a transient exogenous exposure.
The Butyrate Paradox — Applied Therapeutically
The proposed mechanism is that ReBalU restores normal redox decision-making in healthy cells while making hijacked or metabolically abnormal cells less able to hide behind distorted antioxidant systems.
In normal inflamed tissue, butyrate can support NRF2/GPX4 signaling and reduce destructive ferroptosis. In some cancer contexts, butyrate can increase ferroptosis sensitivity by suppressing xCT/SLC7A11-GPX4-linked defenses. This duality is the butyrate paradox applied therapeutically: normal cells receive fuel, barrier repair, and antioxidant normalization, while hijacked cells may be pushed toward apoptosis, ferroptosis-linked vulnerability, immune visibility, or macrophage/T-cell clearance.
Butyrate also strengthens antimicrobial immune programming: researchers reported that butyrate bolstered macrophage antimicrobial activity without inducing inflammation, imprinting an antimicrobial macrophage program. Butyrate can also enhance CD8+ T-cell effector activity and modulate cytotoxic T-cell gene expression — supporting the idea that ReBalU may increase immune clearance capacity rather than merely buffering oxidative stress.
For SOD2 TT/Val-Val individuals, the rationale is especially strong because reduced mitochondrial superoxide handling increases vulnerability when infection, bactericidal antibiotics, hyperinflammation, or oxygen stress raise ROS burden. For CC individuals, the protocol may still improve barrier function, mucosal immunity, DHA resolution biology, and macrophage/T-cell performance — but the TT population is the clearest medical-need subgroup.
Development Pathway
ReBalU is not positioned to replace antibiotics, antivirals, antiparasitics, chemotherapy, immunotherapy, or biologics. It is positioned to identify redox-fragile patients and precondition the host environment so standard therapies work through a more competent immune-redox system.
The platform may be especially valuable where pharma products themselves impose oxidative, mitochondrial, ferroptotic, or immune stress. Bactericidal antibiotics can produce oxidative effects in mammalian cells, fluoroquinolones are linked to mitochondrial toxicity, and gentamicin toxicity is associated with kidney and hearing/balance risks through oxidative-stress mechanisms.
In cancer: ReBalU’s strategic value is as a sensitization and tolerance platform — endogenous butyrate/DHA signaling may protect normal cells, improve immune-cell function, and weaken cells that survive by antioxidant hijacking, ferroptosis resistance, or immune invisibility.
In infection: ReBalU identifies TT/Val-Val and other redox-fragile patients before or during treatment, then supports mucosal barrier function, macrophage antimicrobial activity, T-cell effector function, glutathione/GPX tone, and DHA-derived resolution biology while standard antimicrobials address the pathogen. The strongest claim is improved host tolerance and immune clearance, not direct killing of Y. pestis.
In equity: A pharma-facing study could test whether ReBalU preconditioning changes therapy tolerance, immune-cell function, oxidative-stress biomarkers, and treatment-response markers in genotype-defined subgroups. Because modern evidence bases remain biased toward European-ancestry populations, a test→treat→test protocol that identifies redox-fragile biology directly may be more equitable than assuming one ancestry-derived clinical average applies to all patients.
Closing Statement
ReBalU is a genotype-aware, biomarker-guided endogenous butyrate/DHA platform designed to restore antioxidant decision-making in redox-fragile individuals. Its scientific premise is that pathogens, cancers, and chronic inflammatory states survive by hijacking apoptosis, ferroptosis, immune signaling, and antioxidant control. ReBalU identifies the vulnerable host, restores endogenous butyrate/DHA signaling through the mouth-gut axis, strengthens macrophage and T-cell clearance, and may make hijacked cells more susceptible to standard pharmaceutical interventions while improving host tolerance.
Regulatory caution: This white paper describes a scientific and investigational framework, not an approved claim to diagnose, treat, cure, or prevent plague, cancer, viral infection, parasitic infection, or bacterial disease. Distinctions between proven findings (e.g., ERAP2 plague selection; European-ancestry bias in genomic datasets) and hypothesized mechanisms (e.g., SOD2-redox selection by plague; ReBalU sensitization of hijacked cells) are noted in the text. Clinical claims should be limited to structure-function, nutritional-support, medical-food, or investigational language unless and until controlled studies validate disease-specific outcomes. These statements have not been evaluated by the FDA.